Introduction
Acrylic resin is most commonly used material for fabrication of removable prosthesis, among which heat cure is used widely; acrylic bases attract stains and odor producing organic and inorganic deposits. Plaque is responsible for halitosis and inflammation of oral mucosa in many denture weaeres.[1],[2] So keeping the dentures clean is a strict concern to prevent stains and deposits for a healthy oral environment of the denture wearer.
Various methods of cleaning dentures have suggested.[3] [4] [5] [6] [7] [8] [9] [10] [11] [12] [13] [14] [15] [16] [17] [18] [19] Brushing techniques are the most common method for removing biofilm deposits, it may be ineffective in elderly, lacking motor coordination. Use of ultrasonic cleaning devices is more efficient when combined with denture cleansing agents[20], but are quite expensive and technique sensitive.
Daily use of household cleanser’s, light bleach and vinegar affect on physical and mechanical properties of denture base materials such as tensile strength, transverse strength, solubility and color.
So chemical denture cleansers are preferred over household cleansers, [21] it is easy and effective for geriatric or handicapped patients to handle chemical denture cleansers over other method.
The purpose of this study was to compare the cleansing efficiency of currently commercially available soak type cleansers.
Materials and Methods
Forty healthy subjects were selected among the complete denture patients, treated in department of prosthodontics SDM College of Dental Sciences and Hospital, Dharwad according to following criteria.
1. Patients who have received new complete dentures.
2. Patients having no signs and symptoms of inflammation or infection of oral tissues.
3. Patients who have not suffered from any systemic or debilitating disease.
4. Dentures with good retention and stability, uniform centric occlusion and good finish.
The study conducted on maxillary dentures of the patients, and are divided in to four groups (T1 to T4) 10 patients each (on random basis).
Each group was assigned a particular denture cleanses.
G - T1 was tested for Sodium hypochlorite (0.02%).
G - T2 was tested for Fittydent denture cleaning tablets.
G – T3 was tested for Clinsodent denture cleansing powder.
G – T4 was tested for Cholorohexidine gluconate. (0.2%)
Patient should not use any of the denture cleaning method so as, to have substantial amount of plaque built-up on the dentures.
On the day of visit to hospital, maxillary denture is removed from the patients’ mouth and rinsed under tap water and excess water is jerked off.
Plaque discharge solution (Alpha -plac, Denture products in India) was applied all over the facial and basal tissue surfaces of the denture with the help of cotton pellet and tweezer. The denture was held under running tap water for one minute to remove the excess disclosing solution. After this plaque and stain accumulations on denture were divided into eight groups, four on the facial surface and four on the basal tissue contact surfaces, the polished palatal surface was not included because it is subjected to the cleansing action by the tongue. (Image 1, 2, 3)
The scoring was done using modified Quigley Hein scale
 | Fig. 1 - Denture (food debris, mucin deposit) stained with Alpha-plac disclosing solution before soaking in denture cleanser.
 |
 | Fig. 2 - Denture (food debris, mucin deposit) stained with Alpha-plac disclosing solution before soaking in denture cleanser.
|
 | Fig. 3 - Denture (food debris, mucin deposit) stained with Alpha-plac disclosing solution before soaking in denture cleanser.
|
0 = No plaque
1 = Light plaque (1% - 25% area covered)
2 = Moderate plaque (26% - 50%)
3 = Heavy plaque (51% - 75%)
4 = Very heavy plaque (76% - 100%)
After initial plaque scoring (By summing all quadrant scores), the denture was put in a beaker containing denture cleaner (Depending on test group T1 to T4) and left for 8 hours. (Image 4, 5)
 | Fig. 4 - Denture after soaking in the denture cleanser.
|
 | Fig. 5 - Denture after soaking in the denture cleanser.
|
Then the dentures were re-stained with Alpha-plac disclosing solution and the resultant plaque score recorded. (By - Modified Quigley Hein scale)
The total plaque scores of before and after denture cleansers were noted and the difference of scores were calculated and tabulated.
The results were statistically analyzed to compare efficiency of each denture cleansers.
Reduction in plaque scores after using denture cleansers were analyzed by Wilcoxon’s matched pairs signed rank test. Reductions between the groups were compared by one way ANOVA followed by Duncan’s multiple range tests.
Results
Forty normal healthy complete denture patients were selected for the study. Patient suffering from any debilitating disease, having oral pathosis and/or ill fitting dentures were not included in the study. They were divided into four Groups T1, T2, T3 and T4 of ten patients each, on a random basis.
Group T1 was tested for 0.02% Sodium hypochlorite, Group T2 for Fittydent denture cleansing tablets, Group T3 for Clinsodent denture cleansing powder, and Group T4 was tested for 0.2% Cholorohexidine gluconate.
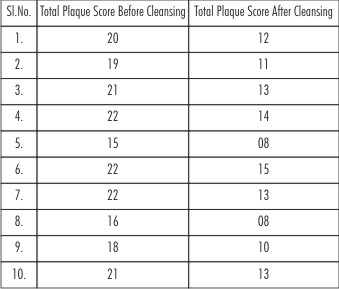
For scoring, plaque and stain accumulation on dentures was divided into 8 groups (4 on facial surface and 4 on basal tissue surface). Reduction in plaque score for each group was compared by taking pre and post cleansing scores. [Table No. 1, 2, 3 and 4]
 | Table No - 1 : Total Plaque score before and after cleansing Group T1 (Sodium hypochlorite 0.02%)
|
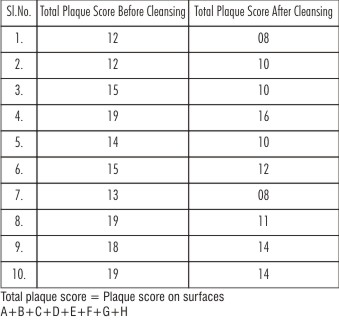
 | Table No - 2 : Total Plaque score before and after cleansing Group T2 (Fittydent Denture Cleansing Tablet)
|
 | Table No - 3 : Total Plaque score before and after cleansing Group T3 (Clinsodent Denture Cleansing Powder)
|
 | Table No - 4 : Total Plaque score before and after cleansing Group T4 (Chlorhexidine Gluconate 0.2%)
|
For Group T1 (0.02% Sodium hypochlorite), means of total plaque scores before and after cleansing were found to be 19.3 and 9.7 respectively. The difference of the means was 9.6 which were statistically significant. [Table 5]
 | Table No - 5 : Group wise mean total plaque score before and after cleansing
|
For Group T2 (Fittydent denture cleansing tablets), means of total plaque scores before and after cleansing were found to be 19.6 and 11.7 respectively. The difference of the means was 7.9 which were statistically significant. [Table 5]
For Group T3 (Clinsodent denture cleansing powder), means of total plaque scores before and after cleansing were found to be 17.8 and 11.3 respectively. The difference of the means was 6.5 which were statistically significant. [Table 5]
For Group T4 (0.2% Chlorhexidine gluconate), means of total plaque scores before and after cleansing were found to be 15.3 and 11.3 respectively. The difference of the means was 4.0 which were statistically significant. [Table 5]
The percentage reduction in plaque scores of Group T1, T2, T3 and T4 was found to be 50%, 40%, 36% and 26% respectively. The percentage reduction was maximum for 0.02% Sodium hypochlorite, followed by Fittydent tablets, Clinsodent powder and 0.2% Chlorhexidine gluconate. [Table 6]
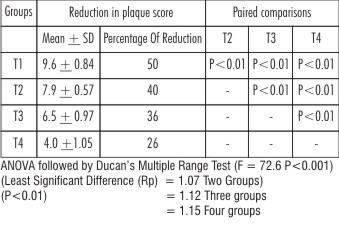 | Table No - 6 : Comparison of reduction in plaque score between different groups
|
The difference data of plaque scores in each of the groups T 1, T2, T3 and T4 was subjected to statistical analysis by using one way analysis of variance (ANOVA) approach. The computed values are presented in [Table-7].
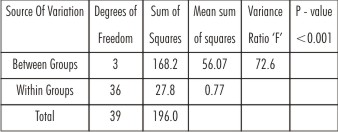 | Table No – 7 : ANOVA TABLE
|
As can be seen from the table of ANOVA, the variance ratio (F=72.6) was highly significant at 0.1% probability level. This indicated that the "between samples" variability was substantially more than the "within samples" variability. This might be taken to imply that the four chemicals were capable of producing considerable differential type of response. The sample data would thus lead us to reject the null hypothesis’ that the treatments are identical in response. [Table 7]
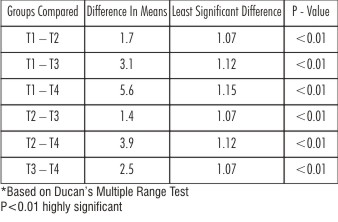
Further in order to identify as to which of the pairs of the treatment were different from one another the "Least Significant Difference" (L.S.D.) at 1% probability level was computed (using Duncan's multiple range test) and the values turned out to be 1.07 for two groups, 1.12 for three groups and 1.15 for four groups respectively. The difference in mean response for each of the six pairs [Table 7] was found to be more than the L.S.D. value which was highly significant. This indicated that for each of the six pairs, the treatments involved in it were different from one another.
Keeping in view the largest mean value of the response and the percentage reduction associated with Group Ti, it might thus be said that 0.02% Sodium hypochlorite proved to be the best (on statistical grounds) out of the four cleansers compared in the present study. The four chemical cleansers turned out to be following a declining pattern in their effectiveness. i.e., Group Ti (0.02% Sodium hypochlorite) was the best, followed by Group T2 (Fittydent denture cleansing tablets), next by Group T3 (Clinsodent denture cleansing powder) and the least by Group T4 (0.2% Chlorhexidine gluconate). [Table 8]
 | Table No - 8 : Comparison Of Mean Reduction In Plaque Score Between Different Groups Mean Reductions T1= 9.6, T2=7.9,T3 = 6.5, T4 = 4.0
|
Formulae Used For Statistical Analysis
 |
|
 |
|
If calculated F > table value ---> Significant simultaneous multiple comparisons (Pair wise)
Duncan’s Multiple range test.
Least significant difference (L.S.D)
Discussion:
Dentures overcome edentulousness which improves the quality of life, which may be harmful when they are not cared from stains and calculus deposited on the dentures and may results in infections of oral mucosa.
In the same manner as on the natural teeth ,[22] the calcareous deposits which form on dentures as consisting essentially inorganic and organic protein (15% to 30% of total deposit), is basically glycoprotein and is responsible for binding deposit on the dentures.
It is presumed that these glycoproteins are similar in nature to the organic matrix of plaque on natural teeth.[23]
There is abundant documented evidence showing the relationship between good oral health and denture cleanliness[24]. A significant relationship between poor denture cleanliness and denture stomatitis was first described by Budtz Jorgenson & Betrum in 1970.[25]
Many soft tissue changes like denture stomatitis, inflammatory papillary hyperplasia and chronic candidiasis occurs due to plaque deposit on the tissue fitting surfaces of dentures. Lack of denture cleanliness, ill fitting dentures and trauma are the most common local etiologic factors for each of these entities.
To maintain good oral health and to prevent tissue from stomatitis and candidiasis like lesions, it is important to keep dentures free from plaque deposit. Infections can best be prevented by oral and denture hygiene.[25]
The present study was conducted on forty maxillary dentures, to know the efficiency of commercially available cleansing agents.
Denture cleanser were[26] used for 8 hrs, and he stated that the efficacy of denture cleansers should be examined under overnight cleansing (6-8 hrs) in addition as recommended by manufacturer.
Observes have compared [27] efficacy of different brands in 20 mints and 8 hrs immersion showed a statistically significant value confirming the past recommendations,[22],[28] that 20 minutes immersion is not enough and that 8 hours immersion is essential for a brand to attain its full efficacy.
The values of mean total plaque score and percentage reduction in plaque score (Table – 6) show a declining trend of effectiveness of cleansing agents used in the study in order that sodium hypochlorite 0.02% was more effective followed by Fitty-dent tablets, Clinso-dent powder and last by Chlorohexidine gluconate 0.2%.
Sodium hypochlorite (Alkaline hypochlorite) will bleach stains and is bactericidal and fungicidal[29]. It dissolves the plaque and inhibits calculus formation by acting on plaque matrix by dissolution of the polymer structure. [22]
The effect of hypochlorite is due to the presence of undissociated hypochlorouscid (HOCL), which oxidizes sulthydryl groups (-SH) of amino acids and proteins to the disulphide form (5 -5).
Sodium hypochlorite (0.02%) was used[30] by overnight soaking of acrylic dentures in 0.02% sodium hypochlorite effectively reduced plaque.
Rudd et al [31] demonstrated effect at sodium hypochlorite as a denture soak. It is known to eliminate denture plaque effectively even after short term exposures[32].
In two separate studies[22],[32] the effectiveness of several denture cleansers in the laboratory. They found Sodium hypochlorite to be more effective than other chemical cleansers used. These findings are in accordance with the present study.
Similarly in other study[33] compared four commercial types of cleansers and found- Clorox (5.25% Sodium hypochlorite) to be more effective than effervescent tablets.
Both fittydent and Clinsodent contains common content that is Sodium perborate which is combined with an alkaline substance such as Phosphate, and when dissolved in water it becomes alkaline solution of hydrogen peroxide.
Upon contact with certain substances, as food debris and mucin on a denture, the peroxide decomposes and produces small bubbles of oxygen which tend to exert a mechanical loosening action between the denture surface and the foreign material.[6],[36],[40],[41],[28],[34],[35],[36]
Chemically, hydroxyl ions of alkalis’ are attracted to the surface being cleaned and neutralize the electrostatic forces between the surface and the foreign material, which allows the debris to become detached and migrate into the bulk of the solution.[28]
The penetration of these ions is aided by the wetting action of a surface active material and consequently, nearly all denture cleansers contain a small quantity of a synthetic detergent. The alkalis’ also exert same chemical action on fatty and protein debris by saponification and hydrolysis.
Cleansing action of fittydent was found to be better than Clinsodent powder which may be attributed to greater effervescence action of fittydent tablets, as when compared to Clinsodent powder.
Alkaline peroxide cleansers are widely used[29] and that they have some antibacterial effect and in addition to the chemical cleansing, they had a mechanical cleansing action due to the bubbles created from release of oxygen.
Effervescent tablets could be useful[21],[27],[34] in an overall denture cleansing program and that they are effective immersion type cleansers.
Disinfectants like (Chlorohexidineglucanate) are not commercially available for denture cleansing, but have been used experimentally to treat and prevent infections on dentures. Immersion of dentures in a diluted solution of cholorohexidine-gluconate, showed a significant reduction in the amount of denture plaque.[25]
Overnight immersion of dentures in a 0.2% solution of Cholorohexidine gluconate prevented recurrence of the infection.
Cholorohexidine is a symmetrical cationic molecule consisting of two 4–Chlorophenyl rings and two bi-guanide groups connected by a central hexamethylene chain. It is a strong base and is more stable in the form of its salts.
Its action is the result of adsorption of cholorohexidine into the cell wall of the microorganism, resulting in a leakage of intracellular components. At lower concentrations small molecular weight substances such as potassium & phosphorus will leach out, exerting a bacteriostatic effect. At higher concentrations, cholohexidine is bactericidal because of precipitation or coagulation at the cytoplasm, probably caused by protein cross linking.
All studies have reported a heavy discoloration of the dentures by cholorohexidine solutions which make this substance unsuitable for routine denture soaking.
Immersion of dentures[25] daily in a dilute solution at Cholorohexidine gluconate caused a significant reduction in the amount of denture plaque and brought about an improvement in the denture bearing mucosa in patients with denture stomatitis.
Peroxide denture cleansers and disinfectants were better than neutral peroxides and crude drugs.[26]
Brushing with alkaline based soap liquid and denture cleansers significantly decreased the amount of subsequently formed plaque. Possibly the potential inhibitory effect of the active agent that persists on the acrylic resin has a better chance of combating the relatively smaller number of organisms likely to adhere initially.[37]
The findings of the present study showed that plaque levels are significantly higher on the fitting surfaces of the maxillary dentures than on the polished surfaces of the denture and teeth. This could be due to pooling of saliva. Denture plaque accumulation is greater in undercuts, rugae areas of the maxillary dentures.
Similar observations were made.[24] in the present study, it was noted that denture surfaces that were convex and smooth appeared to retain less plaque, while denture surfaces that were artistically contoured appeared to retain more plaque.
It was evident that - the findings of the study, all the cleansing agents used were effective for the purpose of cleansing the dentures, on comparison with each other, they were found effective in the following order:
1. Sodium Hypochlorite (0.02%)
2. Fittydent denture cleaning tablets
3. Clinsodent denture cleansing powder
4. Chlorhexidine gluconate (0.2%)
It is apparent that the present study that these soak type cleansers alone may not adequately remove accumulated plaque deposits, especially if the deposits are heavy, so it may be assumed that these chemical denture cleansers are only significant adjacent to denture brushing.
Conclusion:
Within the limitations of the study, on the basis of immersion tests, it may be concluded that these commercial cleansers can be recommended only for the removal of mucin deposited on the denture from the saliva and loosely held food debris, while their daily use may help to prevent the accumulation of heavy stains and calculus, once these deposits have been formed. Some other method is required for their removal.
References:
1. Love W, Goska F, Minon R. The etiology of mucosal inflammation associated with dentures. J Prosthet Dent. 1967;18:515
2. Mc Kendrick ASW. Denture stomatitis and angular chelitis in patients receiving long-term tetracycline therapy. Br Dent J.1968;124:412
3. Ortman LF. Patient education and complete denture maintenance. Dent Clin North Am. 1967;21:365
4. Abere DJ. Post placement care of complete and removable partial dentures. Dent Clin North Am. 1979;23:143
5. Nicholson RJ, Stark MM, Scott HE. Calculus and stain removal from acrylic resin dentures. J Prosthet Dent. 1968;20:326
6. Neill DJ. A study of materials and methods employed in cleaning dentures. Br Dent J. 1968;126:107
7. Mittleman JS. Denture cleaners. J Am Dent Assoc. 1958;56:561
8. Anthony DH, Gibbons P. The nature and behavior of denture cleaners. J Prosthet Dent. 1958;8:796
9. Fleish LM. Care of dentures. J Prosthet Dent. 1960;10:591
10. Ratzow F. Discoloration and cleaning of acrylate prosthesis. Dent Abstr. 1964;9:18
11. Smith DC. Denture cleaners. Dent Pract Dent Rec. 1961;12:93
12. Backenstone WM, Wells JG. Side effects of immersion type cleansers on the metal components of dentures. J Prosthet Dent. 1977;37:615
13. Beck HO. Denture cleansers and retaining devices. J Pharm Assoc. 1973;13:246
14. Muenchinger FS. Evaluation of an electrosonic denture cleanser. J Prosthet Dent. 1975;33:610
15. Budtz-Jorgensen E, Kelstemp J. Enzymes as denture cleansers. Scand J Dent Res. 1977;85:209
16. Myers HM, Krol AJ. Effectiveness of a sonic action denture cleaning program. J Prosthet Dent. 1976;32:613
17. Connor JNE, Schoenfeld CM, Taylor RL. An evaluation of an enzyme cleanser. J Prosthet Dent. 1977;37:147
18. Budtz-Jorgensen E, Knudsen AM. Chlorhexidine gel and steradent employed in cleaning dentures. Acta Odontol Scand.1977;36:83
19. Budtz-Jorgensen E. Materials and methods for cleaning dentures. J Prosthet Dent. 1979;42:619
20. Goodson L.B. A statistical comparison of denture sanitation using a commercially available denture cleaner with and without microwaving. Gen Dent. 2003;51(2):148-51.
21. Kumar M.N. Efficacy of commercial and household denture cleansers against Candida albicans adherent to acrylic denture base resin: An in vitro study. IJDR.2012:231: 39-42.
22. Neill D.J. A study of materials and methods employed in cleaning dentures. Br Dent J 1968;124: 107-115.
23. David C.A. Denture plaque and denture cleansers. J Prosthet Dent 1981:45:376-379.
24. Keng S.B, Lim M. Denture plaque Distribution and the effectiveness of a perborate containing denture cleanser. Quintessence Int 1996;27: 340-345.
25. Jorgensen E.B, Odont. Materials and methods for cleaning dentures. J Prosthet Dent 1979;42: 619–623.
26. Hiroki N et al. Cleaning efficacy of commercial denture cleanser : Ability to reduce Candida albicans biotilm activity. Int J Prosthodont 1995;8: 527-534.
27. Willard T.J. Denture plaque:Quite destroyer. J Prosthet Dent 1982;48:647-652.
28. Anthony D.H, Gibbons P.The nature and behaviour of denture cleansers. J Prosthet Dent 1958;8:796–810.
29. Jagger D.C, Harrison A. Denture cleansing – the best approach. Br Dent J1995;178:413-417.
30. Webb B.C. et al. Candida associated denture stomatitis - Etiology and management: A review part 3 Treatment of oral candidiasis. Austral Dent 1998; 43: 244-249.
31. Robert R.W. et al. Sterilization of complete dentures with sodium hypochlorite. J Prosthet Dent 1984;51:318-321.
32. Moore T.C., D.E. Smith, Kenny G.E. Sanitization of dentures by several dental hygiene methods. J Prosthet Dent 1984;52: 158-163.
33. Mohssen G, Gerland N. Graser, Helmut A. Zander. The efficacy of denture cleansing agents. J Prosthet Dent 1982 48:515–521.
34. Aysun U, Altay O.T, Sahmali S. The role of denture cleansers on the whitening of acrylic resins. Jut J Prosthodont 1996;9:266-270.
35. Mese A. Effect of denture cleansers on the hardness of heat- or auto-cured acrylic- or silicone-based soft denture liners. Am J Dent. 2007;20:411-5.
36. Chethan M.D. MICROBIOL OGICAL EVALUATION OF THE EFFECTIVENESS OF COMMERCIALLY AVAILABLE DENTURE CLEANSING AGENTS. IJDDR.2011, 3 (3): 85-100
37. Sharp E.W, Biol M.I, Verran J. Denture cleansers and in vitro plaque. J Prosthet Dent 1985;53: 584-585.
|